I received an email reminding me the U.S. had reached one million COVID deaths and informing me there are still too many COVID deaths In addition, I was told:
The health care system still is overburdened because the unvaccinated and those who have given up any idea of protecting themselves and others continue to be the primary means for the virus to propagate with over 1.8 million new cases in the last 28 days. No one should be surprised if there is another spike this coming fall. It’s too early to be celebrating anything.
Is it true: we have let down our guard? COVID is still a considerable threat? The unvaccinated are the reason COVID is still a problem?
Our school cancelled the spring sports award banquet due to rising cases (although the kids still attend in person during the day). The school nurse issued a warning too: we are seeing an uptick in positive COVID-19 cases. My wife says the supermarket clientele are growing nervous too; according to her, the supermarket is the ultimate mask wearing haven and mask usage there is increasing.
Are they all rightly concerned? Are we on the verge of another COVID wave? Cases are indeed increasing, but deaths are still declining and near record lows (at 280 per day as of Saturday, May 14). The next COVID twist is impossible to predict; the virus will always be with us and continues to mutate regularly. The current trend is toward less virulent variants, but there are thousands of variants, and the next significant one could be a repeat of Delta or worse. But then again, there could be a virulent flu virus in the next few years; it is the thing everyone was worried about before 2020. Gas prices could rise to $10 per gallon. Did anyone anticipate a baby formula shortage? Any number of other unforeseen disasters could happen; do we all have to take measures to prevent a Pandora’s box of problems or do we reasonably prepare ourselves and basically live our lives as normally as we can?
After all we know now and all the mistakes made, what should we do to prepare for the next COVID wave? Continue to hound the unvax’d, even when evidence of vaccine efficacy shows its impact is quite limited? Continue to panic people so government can extend its power well into the future? Perhaps we should dispassionately looking at the facts instead.
The Numbers
We can now compare three years of COVID results. Throughout 2020 and 2021, the average number of deaths per month fluctuated quite a bit, but the average was consistently close to 40,000 per month over the entirety, slightly more in 2020 and slightly less in 2021.
Total deaths April** – December 2020: 367,444 (40,827 per month)
Total deaths January – December 2021: 478,629 (39,886 per month)
**there were no recorded deaths in January and February 2020 and roughly 5,000 in March 2020.
The wonderful news is that deaths in 2022 are down nearly 25% through the first four-and-a-half months this year as compared to last year:
Total deaths January 1 – May 15 2021: 232,847 (51,744 per month )
Total deaths January 1 – May 15 2022: 175,849 (39,077 per month)
Even better, the downward trend is intensifying. The number of deaths during the last month was 52% lower than it was for this same time period in 2021.
Total deaths Apr 15 – May 15 2021: 20,425
Total deaths Apr 15 – May 15, 2022: 9,657**
*States do not report COVID stats as timely now, so the current analysis is with numbers ending the prior week.
Throughout 2022, deaths have fallen at a (slow but) steady rate, including a 14% drop last week (May 8 – May 14). It is possible to see a slight increase in the next few weeks, but I think it unlikely deaths rise much. Cases have been rising for seven weeks now (from 28,000 per day to more than 100,000 per day), but once the case count slows (who knows when exactly), we will see another significant drop in the death rate. By the time we reach summer, it will be ever-so-clear that 2022 is by far the best year yet.
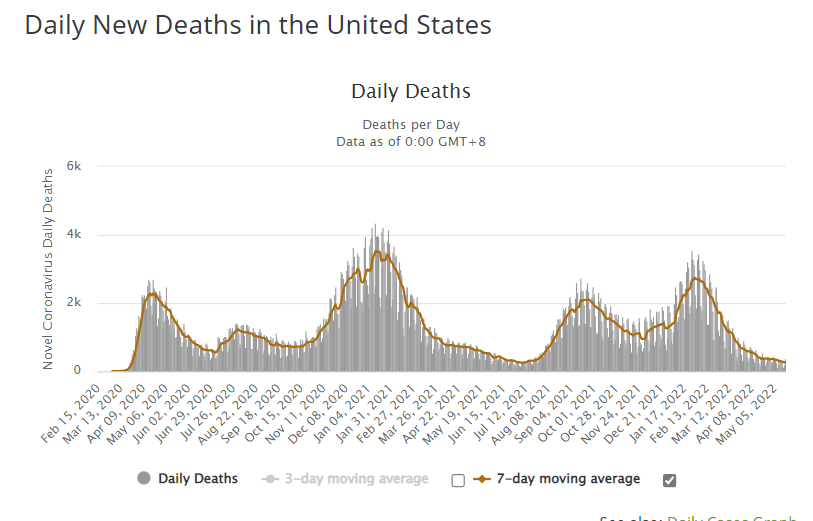
Deaths peaked at nearly 3,500 per day in January 2021. February 1, 2022 they were back to 2,700 per day. By April 16, they fell below 400 per day. May 11, they fell below 300 per day. As of Saturday, May 14, average daily deaths stood at 280 per day.
There have been only 12 days (July 1 – July 12, 2021) when the death numbers were as good or better than right now. The all-time low is 248 per day (July 7, 2021). Throughout 2020, the rate never fell below 500 per day. We are clearly on a better path this year.
The current week could mark the sixteenth straight week of declines. Sometime soon, the U.S. will register its lowest death totals since March 2020. Still, Pollyanna-like optimism is not warranted. My friend did provide one cogent warning:
No one should be surprised if there is another spike this coming fall. It’s too early to be celebrating anything.
I agree we shouldn’t be surprised by anything COVID. We continue to have COVID variants which can run the gamut from mildly to highly virulent, so who knows where the virus is going next? Still, let’s consider the following and lean towards the “glass is half full” argument:
1) the falling death rate: COVID deaths have fallen sixteen straight weeks. We have seen longer drops before, ones which were followed by significant rebounds, but this one appears to be going lower than any of the prior drops, and there is nothing at the moment that signals an upward trend.
2) deaths are falling despite rising case rates: the current week marks the seventh straight week of rising cases. The rate has more than tripled from 28,000 per day to more than 100,000 per day (including more than 120,000 Wednesday, May 18). This is the first time in two+ years we have seen a de-coupling between cases and deaths. Three weeks of rising cases have always been followed by rising death rates–except for this Spring.
3) high levels of natural immunity: 2022 is the year of natural immunity. We relied on vaccines in 2021, but they were mainly a dud (otherwise, explain why deaths did not fall significantly in 2021 and were the same as 2020). 2022 is the breakout year. We have seen a 25% decrease in deaths so far this year because of our reliance on natural immunity (thank God for Omicron!) instead of vaccine immunity.
4) lessening in severity of the virus in the last year. As is painfully obvious, life with COVID is a crap shoot. The virus could have gotten worse, but it hasn’t. It has become more contagious but less deadly. This may be blind luck or it may be a result of evolutionary biology.
5) cases will fall again. So what happens when the case rate flattens and declines (as it surely will)? We have had seven weeks of modest increases. This current rise is much less pronounced than it has been for all the other waves. Once that rate begins to drop, we will see another significant decline in deaths. The relative weakness of this increase, signals that the decline will arrive relatively soon.
6) deaths are falling world-wide–and they have fallen dramatically. Before 2022, total world-wide deaths had never fallen below 5,000 per day and had risen to as many 15,000 per day (a vastly under-reported number in many countries). The current world rate has fallen well below 2,000 per day. This is a harbinger of good things to come for us as well.

All of this could turn around later in the year. We can predict the trends only a little way into the future. In any case, we certainly do not need more restrictions in place when there is no crisis (and perhaps a grand diminution on the way). I ask my friend: what is his solution? Should we take our eyes off the other potential problems that haven’t yet manifested, but are just as real?
We need to watch for rising cases during the summer. Both in 2020 and 2021, the U.S. experienced rapidly rising cases and deaths beginning in early summer, usually driven by the Southern states, as Southerners moved indoors during the hottest months. What will happen this year? This summer’s numbers will provide another indicator of whether we remain in an endless cycle of ups and downs or if we have finally broken through the glass ceiling. Given the current situation, the odds are in our favor, although not certain.
The overwhelming majority of Americans either have natural immunity or are vaccinated. Is COVID going to break through despite these protections? Right now we are in as good of a situation as we have ever been.
Even Bill Gates, Renaissance man and newly discovered COVID expert (per our one-channel media), has come around to some of our points of view. Last week, he finally arrived to the point where many of us were a year ago:
Gates-says-COVID-is-kind-of-like-the-flu
Gates explained, “We didn’t understand that it’s a fairly low fatality rate & that it’s a disease mainly in the elderly, kind of like flu is, although a bit different than that.”
Regarding the vaccines, Gates said, “once Omicron comes along, the vaccine is not reducing transmission, hardly at all, particularly about three or four months after you take the vaccine.”
Welcome back to reality, sir. Mr. Gates even compared COVID to the flu, something that would have had an ordinary conservative kicked off social media, but it sounds like great, new found, wisdom from this wise oracle of the Left.

Talking Points that Won’t Die
My friend noted that the unvax’d are stressing the system, presumably for selfish reasons. He also added:
Around a million U.S. citizens have lost their lives and that didn’t need to happen if certain government officials at the time hadn’t buried their heads in the sand hoping it just would go away, and if people hadn’t been convinced that taking horse meds was a better idea than getting vaccinated.. We can look again at the differences between vax’d and unvax’d.
First, I haven’t seen any evidence that the unvax’d are stressing the system more than anyone else. Even Bill Gates, oft-times spokesman for the lock-down crowd, acknowledged the virus threat is greatly striated by age (this pattern, by the way, was clear in early 2020 despite the befuddlement of Bill Gates).

Those over 50 account for 93% of COVID deaths; senior citizens account for 73% of deaths (these numbers differ marginally from the Worldometer count I typically use).
If you’re over 50, you have incentive to be vax’d (and the vast majority were). If under 50 and otherwise in good health, being unvax’d is not an unreasonable risk. At one point in time, folks like my friend might have been able to legitimately accuse the unvax’d of spreading the disease to the high risk folks, but last year demonstrated the vaccines do not prevent transmission; both vax’d and unvax’d spread it at the same rate. This means if you are unvax’d, you are taking that risk on yourself only. So, why does government force others to take protections they don’t want and are a benefit to themselves only?
If you had the virus previously, natural immunity is working in your favor; it is not at all unreasonable to skip the vaccine or the booster after contracting COVID.
I also don’t see the point of vaccination at all for minors in good health. In fact, for healthy minors, it is quite reasonable to consider the risk of vaccination greater than the risk of COVID itself. Minors account for just one-tenth of one percent (.1%) of all COVID deaths, but healthy minors are a fraction of that fraction. From a statistical standpoint, my two teenage kids have zero risk of dying from COVID, so why would we vaccinate them against a non-existent threat?
By the way, the CDC now is green-lighting the boosting of 5 to 11 year-olds. https://www.cnbc.com/2022/05/19/covid-kids-shots-cdc-panel-recommends-pfizer-booster-for-children-ages-5-to-11-.html.
Only 29% of kids in this age group have been vaccinated; ABC tells us that the low rate is due to cost. Really? Uniformed parents don’t know the vaccine is free? https://abcnews.go.com/Health/Coronavirus. Nope. Wrong again. Do you want to select another answer for half-credit? Is there any wonder the media has lost all credibility with a large chunk of the American public?
Other COVID risk factors include excess weight, diabetes, asthma, chronic respiratory conditions. For these folks, the vaccine seems a reasonable precaution. So, why are the unvax’d the ones who get all the vitriol and disparate treatment when there are many more significant risk factors? The greatest risk is not to the unvax’d, so why target that group alone and not look at all factors? Or why bother to pressure anyone at all in the current environment?
Sometimes, the evidence is too overwhelming even for super cautious bureaucrats to ignore. We see this month that the J&J vaccine is halted for some (a second time for J&J): FDA restricts J&J’s Covid vaccine because of blood clot risk (nbcnews.com). Remember, last year the FDA added a myocarditis warning label to the other vaccines. Remember the FDA originally recommended against boosters for those under 65. Maybe the folks wary about the vaccines last year, weren’t so crazy, after all? Maybe there have been issues with vaccines in the past? Maybe something similar delayed the polio vaccine for seven years? Maybe the swine flu vaccine was halted for similar concerns? Maybe the COVID risk just never was relevant for many young and healthy folks? Or, alternatively, maybe everyone opposed to taking the COVID vaccine themselves are just crazy right-wing conspiracists? You make the call.
The point is that vaccinations are right for some but not all, a point I have stressed continually. Some are willing to assume the risks of vaccinating because of their individual risk to COVID itself, but everyone has their own calculation to make. My friend, I believe, is repeating a talking point that just doesn’t hold water any longer.
My friend referenced “horse medicine” as well. The popular talking point is to describe Ivermectin, advocated by many as a COVID treatment, as “horse medicine”. People with a hidden agenda want to discredit Ivermectin and paint as stupid anyone who deems to take it, but given the facts below, it is not an unreasonable treatment course:
- Ivermectin was a Nobel prize winner in 2015 (for its impact on humans not animals)
- Ivermectin is on the WHO’s list of 300 essential medicines for humans.
- It has a track record of treating disease in humans for more than 50 years. It has been prescribed to humans billions of times.
- It is highlighted as a potential COVID treatment by numerous well respected doctors, including Dr. Pierre Kouri who touted its benefits in Congressional testimony in 2020 (for more on his and other credentialed doctors’ views, see this prior post: vaccine-saftety-who-killed-ivermectin).
- It has an excellent safety record, far better than the COVID vaccines.
- Empirical evidence from around the world (Japan, India, Mexico, U.S,, and others) has shown Ivermectin effective in treating COVID.
Even if it doesn’t work well, why not give it a try? Isn’t that the same argument used by those advocating for the vaccine? It is most telling that they describe Ivermectin as “horse medicine” when it has been used successfully to treat both animals and humans. This sophistry makes their motives suspect. This is done only to make it seem illegitimate.
Certainly, many others believe if Ivermectin were as profitable as the vaccines, it would have been more widely recognized. I don’t know the truth about this, but it is hard to dispute this point.
I know several MDs personally who recommend Ivermectin. One of them prescribed the medicine to me (luckily, I didn’t need it). The last year-and-a-half, I listened to many other highly credentialed doctors who advocated for it publicly. I even know several stricken with COVID who saw remarkable turnarounds after an Ivermectin treatment course. All these data points mean nothing? I am a big dummy for still believing in “horse medicine”? I am basing my hopes on silly internet talking points? Come on. Open your mind just a little bit to see the other side of the argument.
But the talking points regarding the unvax’d and horse medicine are pervasive and will always be accepted by many. In our public discourse today, we have competing versions of the truth, and those who believe an alternative version of the truth are scorned as idiots or bigots or worse (they should be shot for risking others lives, being selfish, for burying their heads in the sand, etc.).
I understand many can be led astray by experts who we should be able to trust and I don’t want to be too harsh on those believing an alternative to my own view. Nonetheless, I also understand the distress of my colleagues who are concerned about the new government policy on COVID testing its unvaccinated employees. Only the unvaccinated are tested, and those who refrained from vaccination see themselves as unfairly targeted. Why the disparate treatment many ask? Where are the metrics supporting this policy? The metrics, in fact, do not support the policy and this is the essential problem: disparate treatment for the vax’d and unvax’d based on questionable metrics.
I raised this issue in a town hall with senior leadership this week, and they gave me the standard talking points. Vaccines work, they say. I didn’t argue against vaccines in the meeting, but I mentioned that natural immunity works great too. In fact, study after study shows it lasts longer and is more effective than vaccine immunity. Why isn’t it considered? I got no pushback to that response.
We should continue to hammer away at the known, established facts, inconvenient facts that so many choose to ignore when making their own points to further their own agenda. Age is a far more significant risk factor than anything, yet it is not considered in any calculation. Why not? Your individual risk factor depends on much more than your vaccine status. If our employer’s goal is to best protect our employees why is only one factor (and not the most impactful one) being considered? I told our senior officials that our colleagues would be more willing to support this policy if the science supported it. It is disparate treatment based on questionable metrics. Folks like Dr. Fauci and Dr. Walensky sell their version of the science to the public, yet so many more, many just as worthy of consideration, contradict their version.
Closing Thoughts
I don’t believe all is lost. There are rules we can follow and often we can turn these rules to our advantage. Play the game effectively when necessary. There are legal options to fight against new policies, and there are many cogent arguments against those who blame the unvax’d and who ply the “horse medicine” mantra. We have had an impact. The fight over vaccinating all government employees as well as most of private industry has been scrapped for now. Those are substantial, if only temporary, victories.
There are still many problems to overcome and the state of affairs in the country is in many ways very sad, but there are definitely signs that things are beginning to commence to start to turn around. In a recent post, I discussed what may be incipient victories in our fight against the insanity: twitter-roe-v-wade-and-the-reopening-of-American-Democracy. I am encouraged by that. It means we shouldn’t quit pushing for positive change, even when we lose a few battles initially.
For more on COVID, the actual facts along with the insanity put in perspective, see: https://seek-the-truth.com/category/covid/
A Little Bit More from an Expert (Late Addition):
The FDA has added a warning label to the mRNA vaccines (for myocarditis), especially for males ages 16-29. The FDA is also now limiting the J&J vaccine (for thrombosis – blood clots). Dr. M says he has seen no cogent argument for vaccinating children. Yet, the CDC now recommends boosting children ages 5-11 and some at our school still want to highlight the point that our kids are not vaccinated.
What do we do when we get conflicting information from different experts? My conclusion after following this closely for two years is that our government experts are influenced by politics and seek to share only information (or to manipulate information) to achieve a desired result. I look instead for those who present information to allow us to decide for ourselves. An open-mind is key. For instance, we should be willing to hear evidence both in favor of vaccinations and those for limiting vaccinations, and not simply be for or against. We should not come to a hard and fast, one-size-fits-all conclusion on the need for vaccinations. The vaccines are clearly limited in their efficacy; they have been oversold and now have some well-established risks. While they are not appropriate for all, it does not mean they have no value for some. Again, each of us to decide what is best given our unique circumstances. This ability to decide for ourselves is what many government officials along with their medical experts are afraid of, and so they seek to limit our access to information. They think we are not capable.
I am highlighting a few of our doctor’s points, but you can read the entire newsletter at the link below. He does not appear to have a hidden agenda and wants to provide as much information as possible to all of us, so that we can make informed decisions.
Link to newsletter: https://visitor.r20.constantcontact.com/manage/optin?v=001xQbTsTOUeGCCuHBIaK9NoqSiCrtJi5d_kvi0-tJS-L8K1JEayZdxQWmPMtfopQ60MJ4FpkexhFqGUrTcYYKSxP-IEbqaboMe22l_ofG55c8%3D
- All signs point to SARS2-Covid infection 1-3 x per year for most of us moving forward. It is the new common cold with a massive bite. Vaccines and boosters will not slow this train as far as the data shows to date.
- (Post Author: As I mentioned above; this is regarding the J&J vaccine) FDA revises the use of Janssen Covid vaccine because of a serious adverse event: After conducting an updated analysis, evaluation and investigation of reported cases, the FDA has determined that the risk of thrombosis with thrombocytopenia syndrome (TTS), a syndrome of rare and potentially life-threatening blood clots in combination with low levels of blood platelets with onset of symptoms approximately one to two weeks following administration of the Janssen COVID-19 Vaccine, warrants limiting the authorized use of the vaccine. (FDA)
- Another important tool the U.S. should add to its vaccine arsenal is Novavax. Novavax is a protein subunit vaccine, similar to flu vaccines and those for many routine childhood immunizations — this more traditional vaccine technology could help some overcome vaccine hesitancy.
- Boosters following vaccination are continuing to show weaker immunity against the variants than natural infection after vaccination. Two new studies noted this effect. We have seen these data sets repeatedly show up over the last year. (Ellis R. 2022) Natural immunity for those that are not at risk seems like a better way to go moving forward.
- This study is of interest because the data again shows limited benefit of boosters on outcome risk in a high risk healthcare population. Memory T cells are a major player in severe and moderate disease reduction and there is no difference in these responses whether boosted or not. Boosters appear to only increase your neutralizing antibodies for a very short period of time in multiple studies, as shown in this newsletter in recent months, which in turn reduces the viral illness rate by 50% during the few weeks following injection.
- Again, we see that the US volume of children with SARS2 immune knowledge is at a minimum 75%. This raises the question of any need for vaccination for any child with a priori exposure. I have seen no data that it would be necessary moving forward for this group to prevent MIS or any other negative outcome. I am waiting for a cogent argument to vaccinate a child that survived SARS2 without a disease concern. If the child has immune weakness concerns or another disease that makes risk of another SARS2 infection problematic, then vaccines likely make sense. Each person must follow the science and risk stratified data.
- More on Boosting. An excellent article by Dr. Paul Offit is worth a full read. Here is a moderate snippet: “What about booster dosing for persons who are younger? One year after the BNT162b2 vaccine became available, studies in the United States showed that a third dose of vaccine also enhanced protection against severe disease for people as young as 18 years of age. Unfortunately, these studies did not stratify patients according to whether they had coexisting conditions. Therefore, it was unclear who among these younger age groups most benefited from an additional dose. Nonetheless, the CDC later recommended that everyone 12 years of age or older should receive three doses of BNT162b2, regardless of whether risk factors were present. (From Post Author: As I mentioned above, the CDC is now recommending boosters for those ages 5 – 11)
- Hospitalization and death remains decoupled from infection volume in the US and now South Africa has published similar data with a population that is less than 50% vaccinated. (Moore et. al. 2022) This tells us that natural infection is leading to immunity that is preventing serious disease the next go round. This is very important. Death and hospitalization is really the metric that matters. Everything else is political theater in my mind.
Yes, indeed everything has become political. The truth, not the agenda of our political affiliations, should be our goal.

One thought on “Are We Surviving COVID Still?”