The COVID delta variant is spreading in the U.S. and other places, but today’s COVID is not the threat it was a year ago because deaths are not rising commensurate with the dramatic increase in cases. This dichotomy needs to be explained and understood.
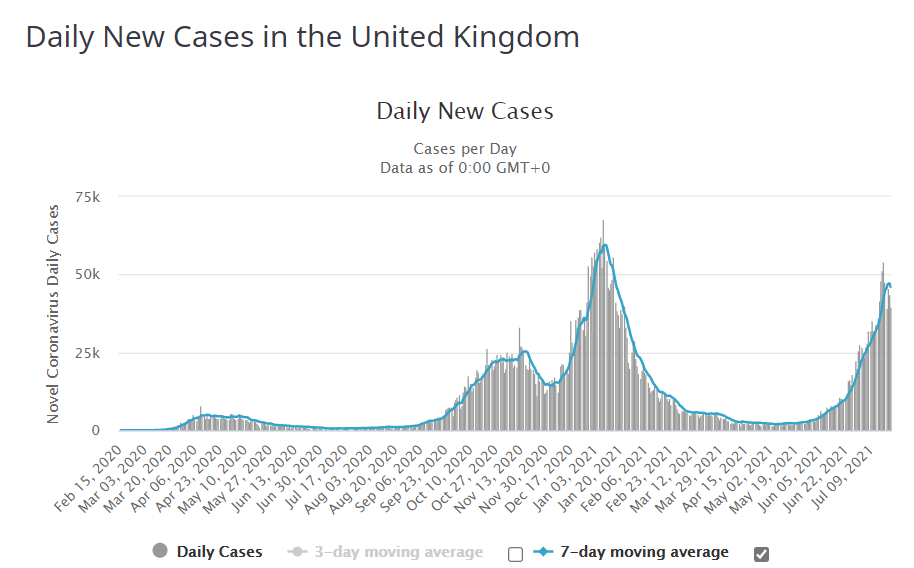
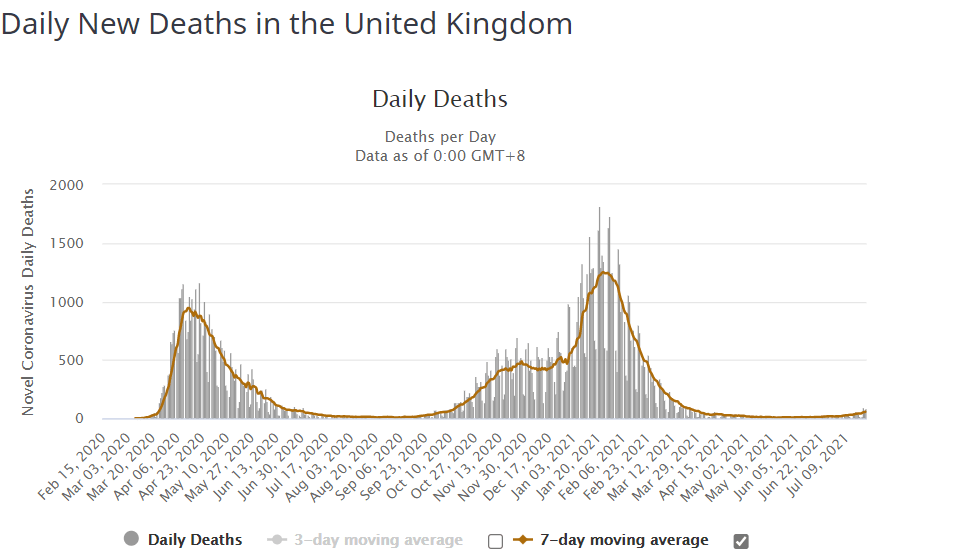
Two weeks ago, I posted that cases in the UK had risen 15-fold (2k to 30k per day) but deaths were only at 25 per day, a surprisingly small number given the dramatic rise in cases: https://seek-the-truth.com/2021/07/10/covid-cmon-man-lets-be-real/. The trend has held the last two weeks. The increase in cases now is 24-fold the last 2.5 months (since May 9) with still a small increase in deaths.
Only during the first two weeks of January were cases in the UK higher than they are today. On January 3, the 7-day average eclipsed 50,000 for the first time in the UK; deaths were 611 per day at that point. On Wednesday, July 22 cases were a hair under 50,000 per day but deaths at 53 per day. In other words, the same caseload in early January wrought 12 times more deaths than in July. The graphs tell this story quite clearly:
It might be hard to detect, but it appears the UK cases are finally flattening with the average having declined this past Thursday and Friday. However, cases are now rising dramatically in the U.S. and Israel, two other highly vaccinated countries, but deaths are still relatively low, still close to the lowest levels they’ve ever been. In Israel, over a four-week period that just ended, there was a single death; four weeks and just one death! The U.S. and Israel got a later start than the UK, but at this point, they appear to be following the in UK’s footsteps. We’ll have to keep watching.
We see this new pattern of very high caseloads and increased replication rates coupled with relatively low death rates, but do we really understand why? I am following the numbers wherever they lead, and the latest numbers are a puzzlement. In fact, this week’s post has more questions than answers because the search for truth sometimes takes time and is not always readily apparent. We can draw some conclusions from the current numbers, but we are in new territory here, so we need to see where the numbers lead in the coming weeks before being certain about more.
First, I have to ask are the vaccines working or are they not? If they are working, why are cases rising so dramatically in highly vaccinated countries? If they are not working, why are deaths not rising significantly while cases are exploding? Dr. Fauci says that 99% of the deaths from COVID today are among the unvaccinated. Can this theory be tested? Can we show once again that the great Dr. Fauci is not at all trustworthy or is he actually right in this instance?
No matter the answers to these questions, remember, right now we are in a better place than we have been since the start of the pandemic. Politicians everywhere are panicking over the rising cases numbers–or maybe I should say they are attempting to panic all of us, but they are not clearly seeing or not sharing the whole picture. The table below illustrates how the U.S. is doing compared to several points in time the last year. Deaths and cases fell steadily from January through June. It looked as if they would continue falling through the summer, but so far in July, cases have risen a mega-whopping 259%. The death rate has also flattened and inched up again, but, as I mentioned previously, the COVID death rate is still well below where it was all of last year and right now it is on par with the death rate from Alzheimer’s and diabetes; nobody is clamoring about deaths from Alzheimer’s and diabetes.
| Date | Avg Daily Deaths | % chg since last period | Date | Average Daily Cases | %Change since Last Period | |
| 26-Jan | 3473 | 11-Jan | 256,210 | |||
| 1-Feb | 3256 | -6.2 | 1-Feb | 148,626 | -42 | |
| 1-Mar | 2003 | -38.5 | 1-Mar | 69,010 | -53.6 | |
| 1-Apr | 919 | -54.1 | 1-Apr | 66,903 | -3.1 | |
| 1-May | 725 | -21.1 | 1-May | 52,604 | -21.4 | |
| 1-Jun | 422 | -41.8 | 1-Jun | 17,481 | -66.8 | |
| 1-Jul | 258 | -38.9 | 1-Jul | 13,874 | -20.6 | |
| 23-Jul | 280 | 8.5 | 23-Jul | 49,800 | 259 |
There is no disputing the numbers. They are what they are. I expect the U.S. death rate will continue rising for a period as it has in the UK the past couple months, but a gradual increase still leaves us in a far better place than we were all of last year and the first half of this year. We are not headed back to where we were a year ago.
I focus on the numbers in this post, but I will address the political aspects of this in a separate post to follow this one; there is much to say about the numbers, but even more to say about the manipulation of the population by our public figures. The COVID deception and dishonesty of the media and our public figures has sunk to a new low this summer. I thought it couldn’t get worse than it already was. Furthermore, their game is not about COVID itself; their actions show they really don’t want to mitigate COVID. COVID is simply a convenient means to other political goals; scare the public, so you can blame your political opponent while you consolidate power that you will not relinquish when this new so-called crisis ends. The numbers are not screaming out for a return to lockdowns or masks or vaccination of the entire population. Our dishonest public figures who are calling for restrictive measures are focusing on one number, the rising cases, but not putting it all in perspective for you.
A Few Questions and Conjectures
On a surface level, the dramatic increase in cases indicates the vaccines are not working, but the tamping down of deaths says the opposite–that vaccines are actually quite effective. If you’ve followed my blog, you know I have been very positive about the vaccines, although these latest data points have me at least questioning their efficacy. I am dubious that the Pfizer and Moderna vaccines are actually 95% effective at preventing illness and I think these data points show that their true efficacy is likely lower than advertised, especially among the variants.
It is also possible that the vaccines have lost steam over time. The flu vaccine is administered annually because last year’s vaccine doesn’t work against this year’s variant; maybe the COVID vaccine has hit the same brick wall? Many experts have said COVID does not mutate as quickly as the flu and that these vaccines should last longer than a year. I’m not a doctor, so I can’t say, but they don’t know for sure either. I’m just asking because the empirical data says something is up.
Nevertheless, I still need more evidence before concluding the impact of the vaccines is anything but a net positive. If that conclusion is where the numbers ultimately lead us, I will follow. Too many folks come to a conclusion and then look only for facts to support their conclusion, but I’ll reverse course if the evidence warrants it.
There are a few more potential explanations for the current numbers that ought to be considered:
- Is COVID spreading among the younger, less likely to be vaccinated, age groups and therefore not killing as many people? I think this is highly likely, although I’ve not seen any stats recently published on the average age of infection. The vaccination rates among senior citizens in the U.S. are close to 90%. The vaccination rate falls off for the younger age groups. Assuming the vaccine is effective, the average age of the infected is significantly lower now and because the average age of infection is so much lower, deaths are also significantly lower. For now, I think this is a reasonable assumption and a plausible explanation for what we’re seeing.
- Are these variants becoming less deadly as they mutate? Can it be the delta variant is highly contagious but no more deadly than the annual flu? This is also a very plausible (although not definitive) explanation as to why cases have risen dramatically, but deaths not so much. The common mindset (dare I say the “herd mentality”?) assumes the mutations will be more fatal and more contagious, more dangerous in general, but this is often not the case. The media dramatizes the latest rise in cases because they want us to pay attention to them, but this does not appear to be last year’s virus at all. A deadly virus that is too effective at killing its victims doesn’t spread as widely because a dead host can’t spread it. Perhaps COVID will go the way of the common cold. Let’s keep watching and test this theory.
- Are the vaccines not quite so effective at preventing COVID, but effective at lessening its severity? This is the claim being made: /https://www.cnbc.com/2021/07/12/most-fully-vaccinated-people-who-get-covid-delta-infections-are-asymptomatic-who-says-.html. I had assumed, as I am sure many of you did as well, that the vaccine would prevent both infections and deaths, but it appears clear now that they are not as effective at preventing infection as originally advertised. Nonetheless, it is not a stretch to still make the claim they are responsible for tamping down deaths. I think this theory is still plausible and time will tell if it is, in fact, the case. Here is another interesting article that seems to contradict this claim at first, but explains that since fewer people altogether dying that the virus is still killing older folks at a higher rate. A fully vaccinated senior is still more likely to die from COVID than an unvaccinated person half their age: https://scitechdaily.com/more-vaccinated-people-are-dying-of-covid-in-england-than-unvaccinated-heres-why.
- Is the vaccine doing its primary function (keeping people alive) and only the unvaccinated are dying? This is what we are hearing from Dr. Fauci, Joe Biden, and others who repeat the statistic that 99% of deaths are among the unvaccinated. I found the following on webmd, which I trust is not partisan, that supports this claim. The article says that during the month of May, 18,000 died from COVID but only 150 were fully vaccinated. https://www.webmd.com/vaccines/covid-19-vaccine/news/20210629/almost-all-us-covid-19-deaths-now-in-the-unvaccinated. The numbers aren’t as good for the UK, because the delta variant has changed the game a bit.
There have been some high profile incidents during which vaccinated people have been infected. More than 10% of the Democrats in the Texas Legislature who traveled to DC recently came down with COVID after traveling on the same plane; this super-spreader event affected all vaccinated individuals. Eight New York Yankees were infected and had to cancel their series with the Red Sox: https://www.marketwatch.com/story/do-breakthrough-covid-19-infections-seen-in-the-yankees-and-bill-maher-mean-vaccinated-people-should-still-wear-masks-11621026068. The UK has 55% of its population fully vaccinated, so you would not expect that cases would skyrocket back to near record levels this month if only a small percentage of those 55% were infected.
As good as they have been, we are now discovering the limits of the vaccines. I believe it is also reasonable to assume that a vaccine designed to fight the original COVID-19 strain would be less effective at stopping a variant of that original strain. We are seeing that in real time. Will the vaccines become less effective as time goes on and there are more variants? We need to wait and see.
Many want simple answers; they often want to put everyone into one camp or the other: either the vaccine is wonderful and we should all have two helpings (damn it all you unvaccinated folks!) or the vaccines are dangerous and no right thinking person should get one (some people like Kamala Harris and Joe Biden vacillate between both camps depending on who the president is today). The truth is the vaccines come with risk and this one appears to be riskier than most (see this thread from Alex Berenson who is reporting on the numbers in the CDC’s Vaccine Adverse Effect Reporting System, VAERS: https://twitter.com/AlexBerenson/status/1388151972096839685), but the vaccines also save lives and the risks are still relatively low.
I can’t tell you how many lives vaccines have saved or if they are the primary factor in holding down deaths in the UK and the US. I conclude we are in a better situation today because of a combination of multiple factors: the average age of infection is declining, variants are becoming less deadly (while at the same time the vaccine is less effective at preventing infection from the less deadly variants), and the vaccine while not necessarily preventing infection does lessen its impact. I have no easy way to tease out and rank each of these factors to determine which is the most impactful, but I am of a mind that they are all contributing to some degree.
The chart below further supports the conclusion that vaccines are effective. I’ve conducted this analysis several times the last month or two and it continues to show that the states with the highest vaccination rates do have lower case rates and lower death rates. This provides assurance that the vaccines are having an impact, although the correlation is not as strong as you would expect if vaccinations were the most impactful factor. For example, we see that the 11 states with the highest vaccination rates (56% and above) have a COVID case rate a quarter (63.98 vs 208.95) of the states with the 10 lowest vaccination rates (40% and below). Similarly, the death rate for the top tier is half what it is for the bottom tier (0.56 vs 1.19)
| Tier | Population | Total Deaths | Death/1M | Total Cases | cases/1M |
| First 11 – 56%-67% | 58,938,216 | 33 | 0.56 | 3771 | 63.98 |
| 2nd 10 – 51-55% | 85,383,655 | 41 | 0.48 | 8090 | 94.75 |
| 3rd 10 – 45-49% | 74,277,587 | 63 | 0.85 | 12263 | 165.1 |
| 4th 10 40-44% | 71,727,503 | 59 | 0.82 | 12,142 | 169.28 |
| 5th 10 34-40% | 37,912,562 | 45 | 1.19 | 7922 | 208.95 |
The difference the vaccine is having is made clear when you split the states into two equal groups, those with rates 48.5% and above, representing half the population, and those below 48.5%. Dr. Fauci said COVID is killing mainly the unvaccinated. I can’t find evidence to dispute that. What I find is that there is a definite correlation between vaccination rates and death rates. It says the vaccine is making a difference. I can’t quantify precisely how much the vaccine improves your individual chances of survival (they are pretty good in any case). This chart tells us if you live in a state with a lower vaccination rate, your chances of dying from COVID are twice as great than if you live in one of the higher vaccinated states (again, your chances are good in either case, but a little better with the vaccine).
| Tier | Population | Total Daily Deaths | Deaths/1M | Total Daily Cases | cases/1M |
| Top Half – 48.5% and above | 159,398,206 | 80 | 0.5 | 20,583 | 129.13 |
| Bottom Half – 48.5% and below | 168,841,317 | 161 | 0.95 | 31,797 | 188.32 |
There is one more factor I deliberately left for last, one that may, in fact, be the most impactful in protecting us from COVID. Interestingly it is also the one factor that gets the least amount of attention from our public figures. For some reason they pretend it isn’t a factor at all (which only adds to my suspicion and distrust of our political leaders). This is also a huge puzzlement for me. See more below.
Natural versus Vaccine Immunity
The U.S. has had 35 million confirmed cases of COVID-19 during the last year-and-a-half. The CDC estimates that the true number, when accounting for unreported cases could be three times higher, COVID-19 infections in the U.S. nearly three times greater than reported, model estimates: Newsroom – UT Southwestern, Dallas, Texas.
There has been debate on whether natural immunity or vaccine immunity is the best, but there seems to be a consensus that both offer protection for a large percentage of people impacted. The U.S. has 49% of its population vaccinated against COVID-19. Approximately 30% of the population has been infected with COVID. There is some overlap in those two numbers (some people have been infected and have also been vaccinated), so we cannot just add the two numbers to determine our herd immunity level, but we certainly have many more than 49% with some form of immunity, natural or vaccine induced. The vaccine number isn’t the whole ballgame, but none of our political leaders nor government medical experts like Dr. Fauci, CDC director Walensky, or the Surgeon General is talking about natural immunity. I cannot understand why. I don’t need to be a doctor to know that something is fishy about this obvious omission. What we need is a number of those who have protection from either vaccines or natural infections or both. We are not being told that number.
So I ask: can we show that natural immunity is having an impact? Is it more or less of an impact than vaccine immunity? Below I look at numbers in the Dakotas, Israel, and Sweden to make a case that natural immunity is a significant factor, maybe even the most significant factor, and that our government officials are being highly negligent, if not totally derelict, in ignoring this factor.
First, North Dakota and South Dakota currently are among the bottom five states in cases per capita (only Michigan, Vermont, and Delaware are doing better) despite being below the national vaccination average of 49% (South Dakota – 46.5% and North Dakota – 39.8%), In addition, for the entire month of July, North Dakota had 10 deaths and South Dakota just five. Per my earlier analysis these two states, especially North Dakota which has one of the lowest vaccination rates, should be doing worse than the states with higher vaccination rates. Together, these two states with a combined population of about 1.5 million are averaging just 4 deaths per week.
So why are these two states doing as well as Vermont which leads the nation with a 67.1% vaccination rate? Why is their death rate on par with the highest vaccinated states? One reason could be that these states rank first (North Dakota) and third (South Dakota) in cases per capita. A higher percentage of their population has been infected, so a higher percentage has developed natural immunity, and hence they are doing better than just about every other state, including most of the states with higher vaccination rates. This argues that natural immunity is a more significant factor than vaccination immunity.
Next, let’s look to a study recently conducted in Israel, https://www.israelnationalnews.com/News/News.aspx/309762
| More than 7,700 new cases of the virus have been detected during the most recent wave starting in May, but just 72 of the confirmed cases were reported in people who were known to have been infected previously – that is, less than 1% of the new cases. Roughly 40% of new cases – or more than 3,000 patients – involved people who had been infected despite being vaccinated. |
Do I need to say anything more: 40% versus 1%? Many doctors offer opinions on which type of immunity is better. The results from this study clearly show which is better. I will take the empirical evidence over the theoretical. Natural immunity is now opening a big lead over artificial immunity.
Finally, let’s look to Sweden. Last year, Sweden was the lone country which eschewed masking and lockdowns; mask-less children attended school in-person the entire year. Sweden bucked the trend and was labeled a pariah because of it. Their strategy was not to prolong the pandemic. Everyone else in the world has done what Dr. John Ioannidis of Stanford warned against in the early days–while attempting to “flatten the curve” they have wound up “widening the curve”, prolonging the pain. Sweden was mocked last year for taking a different approach, but they are doing better than anyone right now. In the month of July, Sweden, a country of almost 10 million with two relatively large urban areas, has had 7 total COVID deaths; that’s less than one death every three days or about two per week. At one point early last year, they ranked in the top ten in deaths per capita, but today they have fallen to 38th world-wide.
Could it be that Sweden is doing well because of their vaccination strategy? Currently, they are middle-of-the-pack at 38.2%, a far lower rate than the UK and the US who are currently experiencing higher per capita caseloads and higher per capita death rates (the UK and the US currently rank 20th and 21st in deaths per capita). So, Sweden is doing far better than would be expected given a modest vaccination rate. Again, as in the case of the Dakotas, it is their high infection rate and their willingness to let the virus run its natural course that puts them in the better position today. Sweden had a lot of infections to be sure; in cases per capita, they rank 12th world-wide, but they are reaping the benefits of their “get the pain behind us early” strategy.
Natural immunity wins over artificial immunity in a TKO.
Children and Vaccines
In his newsletter this week, our pediatrician is now recommending vaccinations for kids 12 and up.
Link to newsletter: https://visitor.r20.constantcontact.com/manage/optin?v=001xQbTsTOUeGCCuHBIaK9NoqSiCrtJi5d_kvi0-tJS-L8K1JEayZdxQWmPMtfopQ60MJ4FpkexhFqGUrTcYYKSxP-IEbqaboMe22l_ofG55c8%3D
1) COVID mRNA vaccines for 12 and over – a few days ago, I had the pleasure of interviewing Dr. Danny Benjamin, Professor of Pediatric Infectious Diseases at Duke University and Principal Investigator on the NC school COVID study, about the COVID vaccine, variants and risk factors for problems in children. He is a brilliant and thoughtful teacher and someone that I truly trust. Our interview will be live in 1 – 2 weeks at the Women and Children First Podcast on Apple podcasts. However, there was one HUGE takeaway that I wanted to share now.
According to Dr. Benjamin, the COVID vaccine has already surpassed the necessary amount of time and number of inoculated children over 12 years of age to steadfastly discuss safety as a net known entity. In the history of vaccine development, there has never been a case of a new unknown side effect being discovered 6 months post any individual vaccination if enough people have been vaccinated to see a signal. As was the case with Rotashield, it took a few years to see the intussusception signal that caused the vaccine to be halted. The mRNA Covid vaccines have been administered to enough children, that we have passed that threshold. According to the CDC over 7 million children have received both doses of the vaccine.
He added a clarification post interview:
There are adverse events, AE, that are: a) discovered “late” in the life cycle of the vaccine (e.g., we did not see myocarditis in the mRNA vaccine until they were on the market 6 months, primarily because young people were not getting the vaccine which is the group primarily affected). This can occur, but is extremely unlikely now because so many people have received the mRNA vaccine. The one caveat is that not many young children have received the vaccine, so this is still possible for children <12. b) the belief that there are AE’s discovered 12 months or 3 years after an individual receives the vaccine. E.g., the delusion that mRNA impacts fertility. This category has not happened in the history of vaccinology.
Based on the weight of the evidence and my trust in Dr. Benjamin, I am now steadfastly recommending an mRNA vaccine for all children that are 12 and older regardless of risk or comorbid health condition. Changing my mind is a reflection of the changing known data sets, safety of vaccination versus contracting the virus and my trust in Danny. I take these decisions very seriously as I impart this information to you. I always make these decisions based on my own children and your child as well. That being said, this is a personal choice and not one that I would force on any one. As always, I am here to help with data and decision making and that is all. Please do not email me if you are upset with my analysis and choice unless you have data that is useful. I know that there are those of you out there that disagree with this assessment and that is ok. Discourse is the key. We are all in this together.
The doctor has been a straight shooter throughout, so I trust his recommendation is based on solid evidence and well thought out, but I have a different calculus for my own teenage kids.
Dr. Benjamin is saying we can now conclude the vaccine risk is very low and should not be a factor in deciding whether or not to vaccinate kids, but the risk from COVID is equally low. Why should we vaccinate our kids against something that is virtually a non-existent threat to them? Only 335 children under 18 have died from COVID in the last year and a half. That’s fewer by half than have died from pneumonia and we aren’t vaccinating our kids from pneumonia. In fact, fewer than 1% of all deaths in children have been from COVID: https://cnsnews.com/article/national/susan-jones/cdc-335-children-0-17-have-died-covid-0673-all-childhood-deaths. By contrast, in the last 18 months, COVID accounts for almost 10% of more of all deaths in those 40 and above.
The risk of dying from COVID doubles roughly every seven years older a patient is. The 35-year difference between a 35-year-old and a 70-year-old means the risk of death between the two patients has doubled five times – equivalently it has increased by a factor of 32. An unvaccinated 70-year-old might be 32 times more likely to die of COVID than an unvaccinated 35-year-old. This dramatic variation of the risk profile with age means that even excellent vaccines don’t reduce the risk of death for older people to below the risk for some younger demographics.
Furthermore, my kids are in good health, participate in high school sports, are not obese, do not have asthma, diabetes, or any other serious health condition or congenital defect that would put them more at risk than the average child. Those additional factors drive their almost non-existent chances of being impacted by COVID down even further. If children were impacted by COVID at a higher rate, it would be an easy decision to vaccinate our kids. We don’t think twice about vaccinating kids against smallpox because smallpox has killed hundreds of millions and your chance of surviving a smallpox infection are not so good, but COVID is a totally different category. So, while Dr. Benjamin tells us the vaccine has been proven safe for kids, is it actually of value for kids, especially for healthy kids?
The lack of benefit is the primary reason I don’t want to vaccinate our kids and this concern wasn’t addressed by Dr. Benjamin. Some folks also say it is important to vaccinate the kids to prevent them from spreading COVID to grandma or their teachers, but many studies have shown that kids are not a vector of transmission, especially asymptomatic kids (in fact, it has never been shown that asymptomatic spread is a problem with COVID). Furthermore, if grandma and Johnny’s teacher are worried about COVID then they should get vaccinated instead of demanding that all the kids be vaccinated.
Finally, while we are hearing that the COVID vaccine is safe; it is still not as safe as the average vaccine. Per the CDC from their VAERS system, the risk from this vaccine are higher than any other has been since they began tracking adverse vaccine impacts, although still not significant enough to outweigh its benefits: https://twitter.com/AlexBerenson/status/1388151972096839685).
When the vaccine benefits to my kids are almost nil, why take a chance at all?

With new cases “rising so dramatically in highly vaccinated countries,” maybe the vaccine is the actual vector of disease. Then the numbers make sense.
LikeLike