Recently, I posed a couple questions to our pediatrician and he has provided responses in his newsletter below. My goal as always is to share as much information as possible, so everyone can be well informed and decide for yourself. Unlike the CDC, your local government officials, Dr. Anthony Flip-Flop, and your social media providers, I trust you with more information.
Link to newsletter: https://visitor.r20.constantcontact.com/manage/optin?v=001xQbTsTOUeGCCuHBIaK9NoqSiCrtJi5d_kvi0-tJS-L8K1JEayZdxQWmPMtfopQ60MJ4FpkexhFqGUrTcYYKSxP-IEbqaboMe22l_ofG55c8%3D
Q: I’ll accept that the vaccines have proven safe for kids, but why should we vaccinate our kids when there is no value to them? (see my post for more: COVID: Do not Panic. Do not Listen to the Politician Behind the Curtain. – Seek the Truth (seek-the-truth.com).
A: Why vaccinate teenagers? A few people asked this question recently. The simple answer is as follows. Although, teenagers are at very low risk for a problem, they are not at zero risk. The safety of the mRNA vaccines is excellent. Is it worth the off chance that your child loses his or her sense of taste and smell possibly for life or worse has a serious myocarditis from a natural infection? I am seeing these types of cases in clinic. It, as always, is a weighing experiment on the scales of risk. I find the risk of natural infection to far outweigh a vaccine event.
It is still a personal choice, but this provides more reasoning for getting kids vaccinated as he is saying deaths are not the only consideration. My wife and I are still in a wait and see mode with regard to the kids, however.
Q: Why do you think there has been so much emphasis on vaccine immunity but not on natural immunity? I think our public officials have been derelict by focusing strictly on vaccine immunity and not addressing the protection we are getting from natural immunity. The doctor provides a reasoning for getting a vaccine after having been infected.
A: A few people are asking about the need to vaccinate if you have already had COVID natural illness. What is the story here? Hot off of the press from Cell Reports Medicine, we see: “Ending the COVID-19 pandemic will require long-lived immunity to SARS-CoV-2. Here, we evaluate 254 COVID-19 patients longitudinally up to 8 months and find durable broad-based immune responses. SARS-CoV-2 spike binding and neutralizing antibodies exhibit a bi-phasic decay with an extended half-life of >200 days suggesting the generation of longer-lived plasma cells. SARS-CoV-2 infection also boosts antibody titers to SARS-CoV-1 and common betacoronaviruses. In addition, spike-specific IgG+ memory B cells persist, which bodes well for a rapid antibody response upon virus re-exposure or vaccination. Virus-specific CD4+ and CD8+ T cells are polyfunctional and maintained with an estimated half-life of 200 days. Interestingly, CD4+ T cell responses equally target several SARS-CoV-2 proteins, whereas the CD8+ T cell responses preferentially target the nucleoprotein, highlighting the potential importance of including the nucleoprotein in future vaccines. Taken together, these results suggest that broad and effective immunity may persist long-term in recovered COVID-19 patients.” (Cohen et. al. 2021)
This builds upon other studies finding very good long term memory B and T cell responses after natural infection especially with increasing severity of the natural illness. This means that in most cases, you are well protected from COVID after a natural infection. However, some RARE individuals will have a low antibody response and may also mount a weaker immune response the second time around as has been shown in some cases. Predicting who these individuals are is not possible at this time on a population basis. Thus, there is a reasonable argument for COVID naturally infected individuals to get one booster dose of an mRNA vaccine to insure a quality response immunologically upon preexposure to the virus. I cannot find any reasonable data or reason to get a two dose series in these people. (Krammer F. et. al. 2021)(Saadat et. al. 2021)(Abu Jamal et. al. 2021)
So the doctor tells us a single booster will provide those with natural immunity extra assurance, although it is probably not needed in most cases. He doesn’t address the concern that our public health officials are not including natural immunity in determining how close we are to herd immunity, but then that one is a political hot potato.
In a prior post, I looked at numbers for Sweden and the Dakotas as justification for touting the benefits of natural immunity. These three all had a high case rates in 2020, but continue to have low death rates despite the delta surge, a fact I think can be attributed to high levels of natural immunity. They still are doing well as of August 3:
- Sweden: had just 9 deaths in all of July and none so far the first three days of August. They are doing better than Israel, a country of comparable population (although more densely populated) which had 55 deaths in July. Israel’s death rate is low because of the effectiveness of the vaccine, but it has double the vaccination rate of Sweden, so natural immunity continues to score points over vaccine immunity (although both still appear to be effective).
- The Dakotas: South Dakota had just 8 deaths in July and North Dakota 11, still among the lowest in the U.S. Between them there has been just one death the first three days of August.
More on Variants
Our doctor also provides more information on the variants. The public is being whipped up to a frenzy over variants, as if we are trapped in a horror movie during which the monsters keep adapting to all that we throw at them, coming back ever more fiercely and ever more deadly; it is only through some unbelievable super-human effort that they are finally defeated. The COVID vaccines do appear to be effective against the COVID variants, but they do have limitations as we see more and more “breakthrough” infections. The conjecture that the variants are less deadly in vaccinated countries (and countries with more infections) seems to be supported by evidence. Life is still good. We are now well into the delta surge, the U.S. is averaging a little over 380 deaths per day, still a 89% reduction from our peak death rate. The current number is also significantly lower than the lowest number from all of 2020. We have public figures running in circles, screaming and shouting, and vilifying all the unvaccinated, but the data seems to indicate that we have beaten back the monster; he is still coming back for more, but in a weakened state. Who knows what the future holds, but the good doctor, in his newsletter, provides us more support for this:
Variants continue to be a HOT and getting hotter topic – SARS2 Version B 1.617.2 Delta is now at 90% of US cases. Data for the delta variant is still showing significantly increased transmissibility (60% higher than the original UK strain). The mRNA vaccines are still working quite well. The breakthrough cases in vaccinated persons with the delta variant have been almost entirely asymptomatic with little to no risk of outcome negativity. There are reports out of Israel that the mRNA vaccines are less effective 39% at preventing infections, however, they remain 88-91% effective at preventing hospitalizations and deaths respectively. This conflicts with the data out of the UK that remains at 88% for any symptomatic disease. (Jones R. 2021)
The DELTA VARIANT IS SIGNIFICANTLY MORE INFECTIOUS THAN THE ORIGINAL SARS2 STRAIN BUT NOT MORE DEADLY OVERALL. It appears to have viral loads a 1000x greater than the original strain as reported recently from China. (Li et. al. 2021) This is important to reflect upon. Until we see a huge uptick in mortality, we can safely assume that our overall risk for a problem once vaccinated even with a breakthrough case remains very very very small. History tells us that these pandemics are rarely if ever shifted into more deadly variants as this offers no advantage to the virus where the increase in spread provides a huge advantage. Remember that the virus only evolves to enhance its survival. Killing the host is not in any circumstance more advantageous.
According to recent CDC documents, the risk of contracting SARS2 once vaccinated with 2 doses is reduced from 186 per 100,000 weekly cases for the unvaccinated to 21 per 100,000 an 8X reduction. Hospitalization is a 25X reduction and death is a 25X reduction. (CDC Site) The take-home point remains that vaccination is the only way to massively reduce risk. As the pandemic rages on again, mask usage in higher risk locales while you continue to practice high quality lifestyle choices will keep the risk to the lowest possible level.
The Lambda variant that started in Peru is now in Texas . It is responsible for over 90% of cases in South America with similarly high transmissibility and similar morbidity to Delta. mRNA vaccines continue to look effective for Lambda despite some poorly sensationalized media coverage stating vaccine failures without making it clear that this data is based on the Chinese vaccine Coronvac. As of this newsletter, I find no evidence that the Pfizer or Moderna, our vaccines, are failing for Lambda. This continues to follow the Delta variant research to date.
There is some news that a gamma variant that is endemic in French Guiana has a high rate of mRNA vaccine misfire or poor efficiency. However, this is not playing out anywhere else yet. This likely leads to a conclusion of a problem of cold storage during vaccine transport and the chain of events leading up to administration. In the US, there have been very few breakthroughs overall at 555 and only 28 were the gamma variant. (CDC) It is so important to follow the rules for vaccine storage, preparation and delivery as this case likely points out.
The effectiveness of the Pfizer mRNA vaccine against the delta variant is 88% according to a new study in the NEJM this week. (Bernal et. al. 2021) This continues to be inline with other studies and is good news for the vaccinated population of the US overall.
Therefore, 12% will have a poorer response allowing for an infection, although likely very mild. Wearing a mask if you are high risk seems to be a really good idea in indoor high risk environments.
All these variants will peak soon and hopefully fade into memory. I say this with confidence by examining the recent history of the delta variant. The delta was originally known as the “Indian variant” (but God forbid we use that term or risk being labeled racists). Cases rose there for nearly two-and-a-half months and then they plummeted, falling just as quickly as they rose. They have leveled off at a relatively low (and dare we hope, sustainable?) level.

We next heard about the delta variant in the UK; again cases rose for two-and-a-half months, slowly at first and then rather dramatically. Since June 21, cases in the UK have also plummeted and not yet leveled off at the bottom. In other words, the UK is following the same happy path as India followed in early Spring.
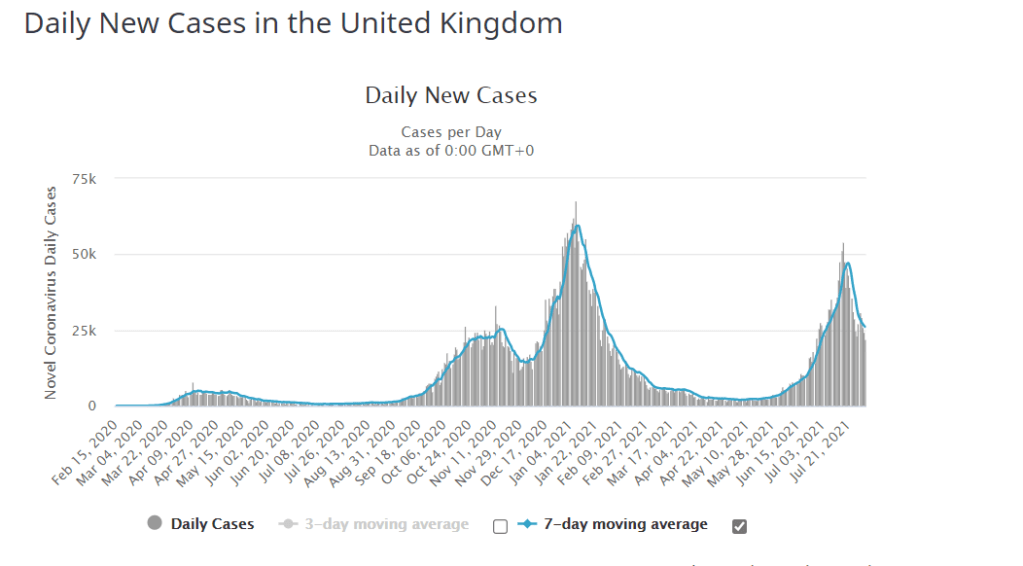
The U.S. and Israel, two other countries hit by the delta subsequently appear to be on the same path as India and the UK. Give us another month or so and we too will get on the happy path as COVID goes into retreat once more. Deaths in the U.S. have risen slightly the last few weeks, but if we follow the path of those other countries, deaths will end up below 500 per day and still below the 2020 levels. The chart below illustrates that the rate of increase in COVID cases is already slowing again:
| Date | 21-Jun | 26-Jun | 3-Jul | 10-Jul | 17-Jul | 24-Jul | 31-Jul |
| Daily Case Rate | 11,789 | 12,558 | 14,653 | 19,710 | 33,518 | 54,020 | 80,637 |
| Percent Change last period | —– | 1.55 | 16.68 | 34.51 | 70.06 | 61.17 | 49.27 |
For the first three days this week, the rate of increase has slowed to 27% (weekly adjusted rate), down from almost 50% last week and 70% three weeks ago. Wait this out just a little while longer; the peak is coming. Unfortunately, our government leaders can’t stop meddling in COVID affairs. You would think they would like to declare victory too, but then COVID can also be used to further other political goals, so they tell us we’re not doing well. Further, admitting that we’ve done all we can at this juncture might just reflect badly on past actions and statements they’ve made.
I wanted to watch more of the Olympics this week and unfortunately ran into Lester Holt on NBC news breathlessly telling us we are all going to die from the delta variant. Hey Lester: there were fewer deaths in July 2021, the month that just ended, than there were any month since the pandemic began. Why are you panicking everyone? I am throwing a 15-yard penalty flag and declaring misinformation on NBC.
In any case, we’ll continue to live in the COVID quagmire for a while longer. Please ask your government officials to stand down unless they have some new information for us, so the rest of us can get on with our lives.
Origins of COVID
The origins of COVID is certainly a topic of interest which I haven’t delved into much. I did note in the last post that Dr. Fauci’s department within the National Institute of Health (NIH) funded “gain of function” research in China and that the head of the Chinese bio-weapons program is now running the Wuhan lab.
Remember too that debate on this topic was shut down by Facebook and other social media outlets last year We Now Know Why Facebook May Have Censored the Lab Leak Theory by Katie Pavlich (townhall.com). Trump was a labeled a racist for suggesting that the virus may have been manufactured in China (something that crossed my mind almost on day one). Now that Dr. Fauci has flipped on this issue and is now agreeing this is a potential explanation for our current predicament, Facebook is no longer censoring and nobody is being called a racist for the suggestion. Meanwhile, Facebook continues to seek new items to censor (which someday may once again be legitimate news). In any case, our doctor shared his opinion in his newsletter, an opinion that a few months ago would have had him banned on Facebook and Twitter:
More on the origins theory of COVID. Katherine Eban and Dr. Peter Attia discuss her investigations into COVID origins on The Drive Podcast episode #169. It is a very deep discussion into the lies, stories, and unknowns related to the start of this pandemic. The end result is as expected. We will likely never know the answer because the World Health Organization, The Chinese Government and the US agencies involved did not do a remotely reasonable assessment of etiology and frankly obstructed the process. Mrs. Eban is very clear that she is not stating a final decision as we cannot without hard science proving a cause. However, the researchers still have not found an intermediary animal nor the index case bat, making the lab leak theory possible if not outright more likely than a natural source in my opinion. The podcast is worth your time purely for the understanding of why each position as to the cause of COVID has merit and where that is.
Vaccine Rates Rising
It seems like the rising vaccination rates should be good news as well. With the delta variant scare, they are creeping back up after falling below 500,000 per day. As of August 3:
In the U.S., 347 million doses have been given so far. In the last week, an average of 681,373 doses per day were administered. source: Bloomberg.com
Are we doing ok in terms of our herd immunity goal? Here are a few stats to consider:
- 70% of all U.S. adults have received at least one vaccine dose.
- 90% of senior citizens (65+) have been vaccinated.
- 50% of the entire U.S. population has been fully vaccinated. Half the U.S. states are at 49% or more fully vaccinated.
- The rate of vaccinations has been rising the last three weeks.
- Every state but one (Mississippi at 39.8%) has at least 40% of its population with one or more dose. All but five (Mississippi, Idaho, Wyoming, Louisiana, and Alabama) are above 45%. This means virtually every state has at least half their adult population with at least one dose.
These number seem pretty good to me. They probably go a few points higher the next couple months. What’s the problem with vaccination rates I wonder? The 12-17 age group is the least vaccinated at just 39%. Maybe our public health officials can beat up on them for lagging behind?
Don’t Forget to Mask Up
Five hundred people have been invited to Barrack Obama’s birthday party on August 4. Let’s see how many of those folks will be masked. My guess is zero, but perhaps I’ll be proven wrong. The Obamas have already exceeded the CDC’s recommendations for the number of people in an indoor event (currently set at 100). Even if they don’t mask up, I am sure they really care about the rest of us. They will join a long line of distinguished mayors, governors, legislators, and Speakers of the House who believe they should follow a different set of rules than the rest of us.
A Reason for Pause
Several of the current COVID vaccines are mRNA vaccines. Dr. Robert Malone, the inventor of the mRNA technology has recently been talking about it. It is interesting to hear his perspective about the limitations of the vaccines, how he believes they should be used, and some of the concerns he has with our current strategy and the ability of doctors and scientists to speak freely.
Dr. Malone is the discoverer of in-vitro and in-vivo RNA transfection and the inventor of mRNA vaccines, while he was at the Salk Institute in 1988. His research was continued at Vical in 1989, where the first in-vivo mammalian experiments were designed by him.
I have been pro-vaccine all this year and I still believe they are doing us good, but I have come to realize there are clearly limitations to their efficacy. I am also aware that there are risks and the current environment of censorship is worrisome. How much about the limitations and risks are being suppressed? No medication comes without risks and limitations. We need to hear the pros and the cons. We need people like Dr. Malone, who knows as much about vaccines and viruses as anyone, to be able to speak freely. We need a debate among the smartest and best in the fields of virology, vaccinology, and epidemiology. We need to seek a range of opinions, including divergent opinions. If the vaccine isn’t all it is cracked up to be, so be it. If it is the modern miracle we have believed it is, then let’s know the whole truth so we can be more certain. Yet, there are too many that want to control the debate; any discussion about the potential risks or the limitations of the vaccine cuts against the message they are trying to send, so they attempt to squelch it and attack the messengers. We need to know the whole story, so vaccines can be used in the most effective manner.
Dr. Malone and the other doctors in the first clip below talk about the problems created by censorship. Doctors who want to raise any concerns about vaccines are being attacked as they were attacked for advocating for HCQ, attacked for questioning lockdowns or masking, and now attacked for raising concerns about the vaccine. Consensus is not required. Let’s hear all of the debate, even if it is a bit messy. We can still promote the vaccine, and Dr. Malone does (but not in the same manner as being advocated by our public officials), without turning a blind eye to the downside. Good work takes time. Let’s take the time to get this right. The stakes are too high.
The Inventor of mRNA Vaccine Technology: Dr Robert Malone – Bing video
Luckily, I found the following video on Rumble. YouTube appears to have censored the last half of the Tuesday’s Steve Deace Show which includes an interview of Dr. Malone (they need a counter like McDonald’s once had for burgers sold; 100 million pieces of information censored, and counting). Apparently, the folks at YouTube believe they know more about mRNA vaccines than the inventor of the technology behind them. I didn’t know they were medical experts too. Go figure.
Advance to the 49 minute mark and listen to Steve Deace’s interview of Dr. Malone (I am sorry, but I cannot find a separate video of just this interview). This is a fascinating and very important interview. If you are a doctor, an expert in this field or just a layman who wants to know more, you will find this worthwhile. He discusses some of the limitations of the vaccines such as the lack of durability of the vaccines, the lack of efficacy in stopping infections and transmissibility (called leaky vaccines), the potential for the vaccines to actually enhance the deadliness of the virus (called ADE, Antibody Dependent Enhancement),our strategy for vaccinations (which he says needs to be more targeted), and something called escape mutants (sounds like science fiction, but apparently is not) along with his own thoughts about the origins of the virus.
A Chaotic Day | Guest: Dr. Robert Malone | 8/3/21 (rumble.com)

Greetings, I do believe your site could possibly be having web browser compatibility problems. When I look at your web site in Safari, it looks fine but when opening in IE, it’s got some overlapping issues. I merely wanted to give you a quick heads up! Aside from that, wonderful blog!
LikeLike