The more evidence that is brought to light that mask mandates, and masks in general, are ineffective at stopping the spread of COVID (or other communicable diseases), the harder the push is to enforce masking in schools, to bring back mandates for the general public, to openly criticize those who favor freedom of choice on the matter (as well as the matter of vaccines), and to generally crack down on people who are following what appears to be the actual science. I see this as mainly a stubborn resistance to facts and data. If COVID lingers on another year or two, will there still be those that tell us how many more lives would have been lost but for masks? This claim that masks have saved lives can never be proven. How many have they saved exactly? But then, the claim can never be disproven to their satisfaction, and so it will be a claim that lingers on interminably. While I understand that many are driven by empathy and emotion and a desire to make things better and do their part, the push for masking is, in fact, not productive. You wear your mask if it makes you feel better, and I will take the precautions that suit me and mine.
If you are one of those who says masks are effective and masks work ask yourself: why do you believe it to be so? Very likely, it is because you are listening to an expert who says so. I share below many experts who say masking is not effective.
Take time to consider the matter and ask yourself what actual evidence has been presented that masks are effective? If you are honest with yourself, the answer may surprise you. Can you actually cite any evidence to support your belief in masking? When the experts don’t agree, and they do not in this instance, you need to dig a little deeper and not just trust what you are told. It is not sufficient to cite the expert (or the political figure) who says what you want to believe, at least it is not sufficient to convince people like me who have dug into this deeper and have some actual facts and science to counter your argument. Have the experts you follow made you aware of any studies showing that masking is effective? Have they provided their reasoning or do they just rely on the fact that they are experts and you don’t need the gory details?
There haven’t been many studies that have concluded masks are effective. The studies we do have often do not measure actual results; studies done in a lab with masks attached to dummies and machines which shoot particle droplets at said dummies are one thing, but empirical evidence is always more compelling. There are some studies which do make claims about masking, but the results are often weak tea or the methodology is not sound.
What Does History Tell Us?
Ask yourself this question as well: is there historical data showing masks have been effective against prior outbreaks? Or did the history of virology just begin with COVID-19 two years ago? Many of you should be old enough to remember the swine flu epidemic of 2009. Do you remember the call for masking during or following that outbreak? I am old enough to remember there was no such call for masking. Was that because the scientists back then not as smart as the ones today? Or were they just less political? Maybe you think the swine flu wasn’t on the same scale as COVID. Think again. There were fewer deaths from the swine flu, but there were actually more confirmed cases of swine flu than there have been for COVID-19 (to date, there have been 40 million confirmed COVID-19 cases in the U.S.):
During the pandemic, CDC provided estimates of the numbers of 2009 H1N1 cases, hospitalizations and deaths on seven different occasions. Final estimates were published in 2011. These final estimates were that from April 12, 2009 to April 10, 2010 approximately 60.8 million cases (range: 43.3-89.3 million), 274,304 hospitalizations (195,086-402,719), and 12,469 deaths (8868-18,306) occurred in the United States due to pH1N1. These final estimates are available at: Estimating the burden of 2009 pandemic influenza A (H1N1) in the United States (April 2009-April 2010)
So, in terms of transmissibility, swine flu can be legitimately compared to COVID. So, what did the experts say about swine flu back then? This is the CDC’s take in 2009:
source: https://www.cdc.gov/h1n1flu/masks.htm
Information on the effectiveness of facemasks and respirators for decreasing the risk of influenza infection in community settings is extremely limited. Thus, it is difficult to assess their potential effectiveness in decreasing the risk of 2009 influenza A (H1N1) virus transmission in these settings. In the absence of clear scientific data, the interim recommendations below have been developed on the basis of public health judgment, the historical use of facemasks and respirators in other settings for preventing transmission of influenza and other respiratory viruses, and on current information on the spread and severity of the 2009 influenza A (H1N1) virus.
In community and home settings, the use of facemasks and respirators generally are not recommended. However, for certain circumstances as described in Table 1, a facemask or respirator may be considered, specifically for persons at increased risk of severe illness from influenza.
Use of N95 respirators or facemasks generally is not recommended for workers in non-healthcare occupational settings for general work activities. For specific work activities that involve contact with people who have ILI, such as escorting a person with ILI, interviewing a person with ILI, providing assistance to an individual with ILI, the following are recommended:
The only instances the CDC recommend face masks is for the individual who is ill or in poor health, not for kids in school, not for those of us shopping or going to the gym, the movies, or out to eat, NOT FOR THOSE WHO ARE NOT YET INFECTED AND IN GOOD HEALTH:
the ill person should be asked to follow good cough etiquette and hand hygiene and to wear a facemask, if able, and one is available
And, I would add, stay home and don’t infect others.
Do you think there was any discussion of masks following other such outbreaks? Have we even had other outbreaks on scale with swine flu and COVID? Well, in fact, we have had several, and not all that long ago. There were three deadly flu pandemics in the 20th century: in 1918, 1957, and 1968, each killing millions, the 1918 pandemic alone killed as many as 50 million. Mask wearing never become a standard during or after these outbreaks, certainly not on scale it has today. Dr. Fauci, even though already a doctor all the way back in 1968, didn’t have any pull for any of these, but he has been in a position of authority as director of NIAID during the last 40 years. During that period, Dr. Fauci has dealt with the original SARS outbreak in 2002 (COVID-19 is considered SARS 2), the swine flu epidemic in 2009, not to mention the annual flu which typically kills tens of thousands of Americans every year. My point is we’ve had a long and storied history with highly infectious pandemics, many worse than what we are encountering today, but despite all these events, and despite Dr. Fauci at the helm for the last forty years, scientists and medical experts were not recommending masking for such contagions, nor were they recommending masks at the start of COVID. But a few months into COVID that all changed. Why after more than 100 years of precedent did we suddenly change course in 2020?
Why the Change?
But it gets “curiouser and curiouser” still; Dr. Fauci’s initial take on masking in February 2020 was that they were not effective against COVID: https://www.msn.com/en-us/news/us/fauci-said-masks-not-really-effective-in-keeping-out-virus-email-reveals/ar-AAKCZ0c. He was joined in this opinion by other medical experts on President Trump’s Coronavirus task force, including CDC Director, Robert Redfield, Surgeon General Jerome Adams, Dr. Deborah Birx, and U.S. Public Health Service Commissioner, Brett Giroir. None of these folks nor any other prominent medical experts advocated for masking last Spring. Lockdowns were the tool of choice initially.
But then the ball started rolling when Dr. Fauci suddenly reversed himself. Masks became the latest fad, and much of the public bought the message. So nobody could accuse him of being incompetent and offering incorrect medical advice at the outset, he said his original assessment was just a little fib. He told us that knew all along that masks would be needed at some point:
The real question you have to ask is why did Dr. Fauci change his mind on masks (as he has so many times about so many issues in the last two years)? Listen below to the doctor’s own explanation about his reversal. He provides assertions, his assurance that what he is saying now is what you can trust. But he provides no new evidence that was not known before 2020. Further, his explanation of why he deliberately misled the public in the Spring is a bit too cute; he wants to paint himself as a hero despite what he calls a lie.
I think he may have been honest initially, but is lying now. How can we know for sure with this man? The man has lied to us repeatedly the last two years. For instance, see his self-serving and ridiculous and deliberately misleading comments on smallpox and polio for instance which I covered in a post last month: https://seek-the-truth.com/2021/07/29/covid-why-do-you-need-that-information/)
This is the expert you want to follow? He is the last I choose to listen to.
Immediately after the swine flu epidemic, the standard was to have only infected and unhealthy people mask and just ten years later, experts now demand that the uninfected, the healthy, as well as the vaccinated wear masks as a precaution. Why the sudden change?
We trust that those who are clearly ill know better than to come to work or school or go out in public until recovered (as is common sense for most of us). So, the only rationale which remains for masking the general public is asymptomatic spread. In other words, COVID must be so different than every other respiratory disease we have ever encountered that those who are infected but have not yet exhibited symptoms (or may never exhibit symptoms) are spreading the disease. But what do the experts actually say about asymptomatic spread and COVID? First, we hear from Dr. Fauci himself along with the World Health Organization:
| Anthony Fauci: Asymptomatic transmission never National Institute of Allergies and Infectious Disease U.S. Director Dr. Anthony Fauci: “In all the history of respiratory-borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is ALWAYS a symptomatic person.” World Health Organization Emerging Diseases and Zoonosis Unit head Maria Van Kerkhove said coronavirus transmission by people who aren’t showing symptoms is “very rare.” She spoke at a briefing in Geneva. |
source: https://www.israelnationalnews.com/News/News.aspx/286920
Fauci reversed himself later (as he often does). In June of last year, he started playing up the notion of asymptomatic spread: https://nationalfile.com/fauci-promoted-threat-of-asymptomatic-spread-in-public-but-downplayed-it-in-private-email/. But what evidence did he provide for changing his opinion? Again, he never says. He is the expert, so trust him. He is science incarnate. But, again I would like some facts and data please. Here is a study from December 2020 that concludes COIVD spread is no different than every other communicable respiratory disease we’ve ever encountered.
The conclusion is not that asymptomatic spread is rare or that the science is uncertain. The study revealed something that hardly ever happens in these kinds of studies. There was not one documented case. Forget rare. Forget even Fauci’s previous suggestion that asymptomatic transmission exists but not does drive the spread. Replace all that with: never. At least not in this study for 10,000,000.
Well if asymptomatic spread is not a thing, then why mask up? The whole rationale for mask mandates fall apart at that point, so we need to lie about asymptomatic spread if we want to continue the mask mandates. Dr. Fauci doesn’t seem to care that he reversed himself on this issue either, nor does he care that some noticed that held two different positions, one in public and another in private. Maybe he doesn’t care who notices his contradictions and misstatements as long as he continues to hold sway over most of the public.
I think all these data points make sense only if you come to the following conclusion: there was a general scientific consensus after all those outbreaks over the last hundred years that masks are not effective at stopping virus spread. Why else have we eschewed them for so long? Why else in 2009 after the extremely contagious swine flu did the CDC continue to downplay their efficacy?
Certainly, we should all be open to changing our minds as we learn new information. But what new information did we learn between March 2020 and June 2020? What is it that dramatically reversed more than 100 years of established precedence? This is the problem I have with masking. The rationale is not there. I am willing to change my mind, but no real logic or calculus has been provided, certainly not by our dear leader, Dr. Fauci. We need a reason, a very compelling reason, to overturn the precedent that had been established, but no evidence has been provided. What do we know today that we didn’t know two years ago? That has never been explained–because there is no good answer.
The mask theory does sell, however. It just seems like a good idea to wear a mask. Sure, it just seems like common sense. Plus, everyone can do their little part to help and we all feel good about ourselves. That’s fine. But I need more evidence. We’ve never done this before. Why now? I need some real science, and when none is provided, and the real reason appears to be political, I get suspicious.
Let’s fast forward to 2021 and let’s hear what the experts are saying today. Has everyone else fallen in line behind Dr. Fauci? Perhaps he has convinced the rest of the medical community to take another look at masks, if not the rest of us?
Dr. Robert Redfield, CDC director through January 2021, doesn’t seem convinced. He complained about the lack of evidence to justify masking kids in school this Fall:
Redfield then took aim at CDC guidance on masking children in school and if there were studies to back up their recommendation, saying the policy should be “grounded in data rather than opinion.” source: https://www.foxnews.com/media/former-cdc-director-redfield-masking-children-must-be-grounded-in-data-not-cdc-opinion
In the meantime, the White House response to all this was to reach out on Tik-Tok. Unfortunately, there wasn’t much science to share in this video (and not a lot of mask wearing either I should point out): https://www.hitc.com/en-gb/2021/08/10/white-house-intern-tiktok-video/?amp
Dr. Scott Atlas of Stanford University, also a member of President Trump’s coronavirus task force along with Dr. Fauci said the following in an interview: “There is no good science on general population, widespread, in all circumstances, mask wearing.” https://video.foxnews.com/v/6180319589001#sp=show-clips. Was Dr. Fauci aware of this?
A few months ago, Fauci said it makes sense to double-mask. If one mask doesn’t do the trick, try two. Why not three or four? More is always better right? Well, when that idea didn’t take hold, he backed off that notion. In his latest interview this month, Fauci was asked: what is the best mask? “Just wear a mask, any mask” was his response. All masks are good: the mask that has been in your back pocket the last week, the mask you’ve slobbered over the entire day, the mask you forgot to wash last night, the mask the nice lady at the front desk breathed all over before she handed it to you; it doesn’t matter if it is a paper mask, clothe mask, N-95, or duct tape; just wear a darned mask for goodness sake.
But also this month, around the same time Fauci was providing this latest nugget of wisdom, Dr. Ezekial Immanuel, former Biden medical advisor (and architect of Obamacare, by the way) was saying you really need to wear an N-95; cloth masks are not effective https://www.breitbart.com/clips/2021/08/11/ezekiel-emanuel-simple-cloth-masks-are-not-good-enough/. He is joined in this opinion by Dr. Michael Osterholm, another former Biden advisor said the same thing this month: https://mnfan.org/2021/08/18/mn-dr-osterholm-cloth-face-coverings-arent-enough-to-combat-covid-only-n-95/.
Did any of you know that an N-95 is only supposed to be worn once and then discarded? Did you know that training is provided to medical personnel on how to properly don an N-95 mask? Clothe masks, per several of today’s experts and almost all the experts from yesteryear, are ineffective, and N-95 are not practical for most. Don’t worry that the seat belt doesn’t clasp. Just hold it across your body; it may still do some good. Furthermore, did you know that most N-95 masks protect only the wearer? Unless the mask has a double filter, the infected wearer of the N-95 is breathing out COVID particles.
Fauci is even contradicted by himself on the email as was shown when copies of his private emails were obtained through a Freedom of Information Act (FOIA) request. https://nypost.com/2021/06/03/fauci-emails-show-his-flip-flopping-on-wearing-masks-to-fight-covid/
And why don’t masks work? Air slips through the side of the mask. Most masks are not tight fitting and there are gaps (infinitely large gaps from the perspective of the virus particles) along the sides of the mask, and the air you breathe in follows the path of least resistance. Air also slips through the mask itself; it has to because you couldn’t breath well otherwise, and microscopic virus particles can easily penetrate clothe and paper masks.
Furthermore, the virus particle doesn’t stay in a bubble six feet away from the person who exhaled. it Anyone who has studied science knows that the air around is a sea; objects float in this sea of air just like boats and corks float in the ocean or like dust floating in your attic. This is why you are much more at risk inside than you are outdoors. Whenever inside, you are traveling through a literal sea of pathogens. Unless you have a tight fitting mask and use it properly and use it whenever inside, you’re not getting benefit from the mask. Good ventilation to clear the pathogens and good hygiene and common sense on your part will make more of a difference.
Censorship
Dr. Scott Jensen was one of the first to push back on Dr Fauci’s advocacy for masks last year. … https://www.pressradar.com/scott-jensen-attacked-for-joining-lawsuit-to-halt-covid-19-vaccines-for-kids/).
Dr. Jensen was subsequently threatened with removal of his medical credentials because of his audacity to speak out (https://bringmethenews.com/minnesota-news/dr-scott-jensen-says-hes-being-investigated-by-medical-board-for-spreading-covid-19-misinformation, https://www.breitbart.com/politics/2020/07/21/minnesota-sen-dr-scott-jensen-under-investigation-after-criticism-cdc-classification-virus-deaths/. This is another clear signal that the science of COVID has become political.
America’s front-line doctors, a group of a couple dozen doctors, spoke out all last year as well. https://www.lifesitenews.com/news/group-of-doctors-masks-are-completely-irrelevant-to-blocking-covid-19/.
Social media reflexively de-platformed and censored the group. Media Matters and other progressives immediately attacked the group and continue to try to discredit their members because they don’t like contrary opinions https://www.mediamatters.org/coronavirus-covid-19/americas-frontline-doctors-vector-dangerous-covid-19-misinformation.
This is more politicization of science; contrary opinions are misinformation because we don’t like the message, just like was told to Copernicus, Galileo, Columbus, Socrates, and so many others throughout history.
The same scenario played out when a consortium of doctors, Evergreen Medical Clinic, in Evergreen, Oregon spoke out. This past January, they posted an epic criticism of masks; it was immediately removed by social media, but then the Facebook medical team knows more about medicine than hayseed doctors from the boonies of Oregon. I would provide a link to their post, but I am not sure if it has ever has been restored. I saved the original post in any case; see the final section below. Here is a short snippet from that post; it highlights their concerns with recent masking studies:
All studies are not equal. The gold standard of medical evidence comes from randomly controlled studies. Recent observational studies that were used to support mask mandates were poorly designed for confounding factors, carried out in medical environments, and then, impressions were extrapolated to the general public. Studies that evaluated the viral exposure of mice in a cage covered with mask material vs. caged mice without a mask cover does not seem to translate well to a world of humans who use their hands. In contrast, a recent Danish mask study of the general public that was performed in a prospective, randomized fashion did not endorse the current majority narrative and was vigorously criticized and suppressed by some.
Logic argues against mask effectiveness. The size differential between viral particle or droplet size expelled from the human respiratory tract compared to the filter size of surgical or cloth masks is substantial. If you read the fine print on most consumer masks, one will likely read a statement such as this; “not intended for medical purposes and has not been tested to reduce the transmission of disease”.
Empirical Evidence:
Some of the doctors I quote above didn’t pooh-pooh masks totally. Redfield was actually a big advocate for masks last year, but now even he is demanding more evidence for the CDC’s masking recommendations. Osterholm and Atlas also say there is a place for masking, but recognize they play a very limited role. However, Fauci’s guidance: pick a mask, any mask doesn’t, double-mask, mask forever, and so on, doesn’t make much sense at all, not to me and not to his many of his medical colleagues. Fauci is the expert I trust the least.
The best case to be made against mask mandates is real world data. While some studies have concluded that mask wearing is helping ever-so-slightly (I share a few of these below), the real world data shows that COVID rises even when mask mandates are applied and falls even when they are lifted. Outside of vaccines, no public mandated mitigating measure has slowed down the progression. After 18 months of lockdowns, curfews, and mask mandates why do you still believe those measures are helping? The measures individuals take to protect themselves matter more. You want to mitigate the risk, take the precautions which are appropriate for you.
My wife, my kids, and I have worn masks only when absolutely required (e.g. at school, in doctor’s offices). We go about town as normal and engage with others regularly, yet none of us have contracted COVID to this point. The poor slob mentioned below got COVID despite constant mask wearing and living like a hermit. But he is not alone; I know several folks who contracted COVID despite religious mask usage; you may as well.

But let’s move beyond the anecdotal; a CDC study found that more than 70% of those infected with COVID wore masks frequently. Even the so-called liberal fact checkers who blindly support any Leftist cause, admitted this:
It’s true, as the post claims, that 70.6% of the “case patients” self-reported always wearing masks. But an even higher percentage of the “control patients” who did not contract the virus self-reported always wearing masks, at 74.2%, which suggests that their mask-wearing may have helped stave off the virus.
So, at best mask wearing provides a minimal protection: 74.2% vs. 70.6% is not much of an advantage. At worst, they make no difference or, as I have noted in prior posts, they can actually be counter-productive, actually enhancing the risk from other pathogens or adding new risks, especially for young children.
Back in March, the CDC published another study concluding that mask mandates had reduced hospitalizations and deaths. The impact again was minimal at best. https://www.cdc.gov/mmwr/volumes/70/wr/mm7006e2.htm.
This study was published months after they issued their guidance and I believe it was done to save face; given the politicization of COVID, the result was likely a forgone conclusion. I include another link which debunks the CDC study: https://www.aier.org/article/the-cdcs-mask-mandate-study-debunked/
Just this month, Duke University’s Dr. Danny Benjamin and Dr. Kanecia Zimmerman, published a study stating that masks can prevent transmission in North Carolina schools. However, this study had a remarkable statement which I think invalidates it completely:
We don’t have data from within North Carolina as to whether or not, in school in K-12, what happens when children are not masked.
source: https://today.duke.edu/2021/06/research-finds-masks-can-prevent-covid-19-transmission-schools
Basic statistical studies require a control group, a group that does not receive the prescribed medical treatment (or receives a different treatment). In other words, the study needs one group which wears masks and another which does not; only then can it determine which group does better (or if there is any difference at all). How can you conclude masks work well when you don’t know what would have happened if they were not used?
Let’s contrast the Duke study with some empirical evidence that compares two distinct masking policies. After the most recent uptick in cases due to the delta variant, many California counties re-issued mask mandates. We have the perfect experiment now as Orange County (home to San Diego) did not re-issue a mask mandate while Los Angeles County did. Both counties are large urban areas and not too far apart from each other; it seems reasonable to compare the two. So, was there are difference in case rates and death rates?
The results below are from the week of August 22-28. LA county, which imposed mask mandates, had almost double the cases (per capita) and more than double the deaths (again, per capita) than Orange county, which imposed no mask mandate. Go figure.
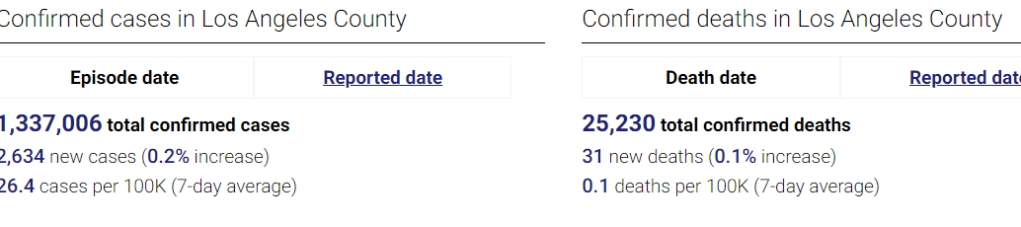
Compare to Orange county.

In prior posts I talked about several places that lifted public mandates. Georgia was the first state to lift mandates last summer. They were promptly condemned as engaging in human sacrifice: https://www.theatlantic.com/health/archive/2020/04/why-georgia-reopening-coronavirus-pandemic/610882/. Today, Georgia ranks 16th among the states in deaths per capita, well below states like New York, New Jersey, Connecticut, and Massachusetts which have had much stricter mandates.
Earlier this year, Texas and Mississippi lifted mask mandates as it appeared the risk of COVID was diminishing. President Biden called their governors Neanderthals. Dr. Fauci and many other political figures also called them out for their heartless action. In the ensuing month, cases in both states fell dramatically. How could that be?
On June 19 of this year, during the height of their deadly delta onslaught, the UK lifted their mask mandate. Again, disaster was predicted. Two days later, on June 21, COVID cases began to fall and continued falling for many weeks. Really? How is that?
The reverse is true as well. I won’t list all the instances in which mandates were instituted, extended, tightened, etc. while cases continued rise; the examples are legion. The virus is gonna do what the virus is gonna despite our mask mandates.
If you want to wear a mask because you think you are helping or you have a medical condition which makes you more susceptible, then please wear your mask, but recognize that many of us don’t see the need. We are not heartless suicide bombers (as has been suggested); we care about our fellow citizens and we care about the truth. The truth, not a lack of empathy, leads to our opposition to mask mandates.
Evergreen Post
Censored post from Evergreen, Oregon, doctors (posted 1/25/2021). Why is this information considered dangerous? Why does Mark Zuckerburg want to stop you from reading it?
We have purposely avoided directly confronting the issue of masks because it is such an emotional and political issue. Like waving a red flag in front of a bull, the topic elicits strong emotions which overwhelms reason. We wear a mask in the hospital and don a N95 mask, gown and gloves when we see a patient known to have COVID-19. Masks are used for source control when patients are admitted with various types of infectious respiratory diseases. After the visit, we dispense of the gown, gloves and change into our regular surgical mask to continue patient rounds. In public, we wear a cloth mask to comply with executive orders and as a courtesy to others who feel afraid and uncomfortable. Like most of you, we rarely wash the mask, we stick it in our pockets, pick it out of the glove compartment or off the floorboard when we need it.
In truth, we wish masks worked. If they did, it would be a cheap, and easy way to control the spread of Covid. The idea that they protect not only their wearer, but also those people around them seems noble. We wished masks worked because citizens are spending billions of dollars on them.
We wish masks worked because most Americans wear them now. Telling them it was unnecessary will not make them happy. We wish masks worked because they have become a symbol for virtue and social responsibility. Anyone who doubts their utility is personally attacked; as though they don’t believe the viral pandemic is real, or don’t care about those who die from it.
We wish masks worked, because they distract from other important Covid related issues such as: school closings, lack of access for non COVID related illness, increased mental illness, elderly dying alone, missed youth experiences, substance abuse, suicides, increased poverty and homelessness, suppression of free speech, censorship of science, disruption of supply chains, government agencies used to oppress small businesses, restriction of religious gatherings, travel disruptions, isolation protocols, modeling over actual data, quarantines, lockdowns, contact tracing, and global harm of the economy that most impacts the working class, vulnerable and poor.
We wish masks worked.
But they don’t.
At least, not the cloth and surgical masks you see in the public arena. They litter the landscape and waterways. They are difficult for people with disabilities and small children. It promotes natural germaphobe tendencies and indoctrinates the young to see their fellow humankind as a sack of germs.
There have been many randomized controlled trials (RCT) and meta-analysis of previous studies that suggest that masks do not work to prevent influenza- like illnesses, or respiratory illness transmitted by droplets and aerosol particles – like Covid. This knowledge was the basis for the WHO and CDC recommending against the public wearing masks in the spring of 2020. It was repeated by authorities and experts at every level.
Dr. Jerome Adams, the Surgeon General tweeted, “Seriously people – STOP BUYING MASKS! They are NOT effective in preventing the general public from catching Coronavirus”
Dr. Anthony Fauci told 60 minutes, “There’s no reason to be walking around with a mask”.
In April, the New England Journal of Medicine wrote: “we know that wearing a mask outside of health care facilities offers little, if any protection from infection”.
What changed? Well, it wasn’t the science.
All studies are not equal. The gold standard of medical evidence comes from randomly controlled studies. Recent observational studies that were used to support mask mandates were poorly designed for confounding factors, carried out in medical environments, and then, impressions were extrapolated to the general public. Studies that evaluated the viral exposure of mice in a cage covered with mask material vs. caged mice without a mask cover does not seem to translate well to a world of humans who use their hands. In contrast, a recent Danish mask study of the general public that was performed in a prospective, randomized fashion did not endorse the current majority narrative and was vigorously criticized and suppressed by some.
A new drug, medical product or procedure would never be approved based on this type of evidence.
Logic argues against mask effectiveness. The size differential between viral particle or droplet size expelled from the human respiratory tract compared to the filter size of surgical or cloth masks is substantial. If you read the fine print on most consumer masks, one will likely read a statement such as this; “not intended for medical purposes and has not been tested to reduce the transmission of disease”.
The best studies are outcome based and measure “patient oriented evidence that matters.” A pharmaceutical company may show their statin drug greatly reduces cholesterol and science can show a correlation between cholesterol and heart disease. So, the obvious premise is that lowering cholesterol reduces risk of heart attacks.
Except it doesn’t. At least not for primary prevention in patients without preexisting vascular disease. It is why you must do the study. Does the intervention work in real world conditions?
In August, Pew Research reported that 85% of Americans said they wore masks in public all or most of the time. If this is so, and if masks are effective, why has the incidence of SARS-Cov-2 increased so rapidly? Why is there not a favorable correlation between mask usage and disease transmission in countries and states with different mask policies?
If masks and lockdowns work, why don’t they work?
The graph below shows the daily number of deaths per million in the UK, France, Spain, Italy and Sweden from March to December. The number to the right reflects the percentage of the population that report wearing a mask in public spaces. Sweden has the lowest number of deaths per million in this comparison despite only 7.7% of the surveyed population reported wearing a mask. For those who argue that Norway, Denmark and Finland have lower mortality rates than Sweden. They would be correct, but these countries also have much lower rates of mask use compared to other European countries (less than 50%). Masks have been oversold as a solution.
Dr. Anders Tegnell, Sweden’s state epidemiologist said, “face masks are an easy solution, and I’m deeply distrustful of easy solutions to complex problems”. He was right. Sweden now (1/23/2021) has fewer deaths per million people (1086) than the United States (1284). In fact, they have a lower death rate than 30 of our states. History is replete with examples when politics or religion meddles with science and adversely impacts solutions. Dr. Martin Kulldorff has argued against widespread public mask mandates from the beginning. He is a professor at Harvard Medical School and a leader in disease surveillance methods and infectious disease outbreaks. He describes the current pandemic policy of COVID lockdowns and mask use this way; “after 300 years, the Age of Enlightenment has ended.”
At this point, many do not need an expert opinion to trust their own intuition and lying eyes that masks are not working. Everyone wants to mitigate the transmission of the virus, but let’s focus on what works.
But, wearing a mask is so easy to do. Can’t you just shut up and wear the damn mask?
Why are we poking this tiger, this mask issue now?
Because there is mass hysteria, and many are blind to it.
Because it’s an irrational and divisive policy when unity is required more than ever.
Because evidence should matter.
Because in 2019, if we saw a father struggling to muzzle a terrified, crying 2-year old child on a plane with a cloth, we would report them to authorities for possible child abuse. In 2021, we kick the whole family off the plane unless the father is successful in his efforts.
Because of a young man with autism who is unable to tolerate a mask on his face is publicly shamed.
Because the masks offer a false sense of security and may adversely impact more important public health mitigation measures.
Because our local high school cross-country teams should not be running the trails wearing masks.
Because the Oregon Board of Medicine suspended the license of a physician who objected to this policy.
Because one of the greatest losses in this pandemic has been the loss of credibility of organizations for whom we held in high regard. Organizations such as the CDC, WHO and Public Health Organizations that need to maintain the trust of the citizens.
Because it is increasingly apparent that the basis for the mask mandate is not medical, but political.
Because fear and panic should not prevail over actual evidence, even when many powerful institutions have expended so much political capital promoting the wrong policy.
We wish masks worked.
We wished we didn’t have to fight about them.
But they don’t.
And we do.
Tim Powell MD
John Powell MD

To mask is the best. Thank you 😊
LikeLike
Spot on ! Thank you. Yours, Baldmichael.
LikeLike